Dizziness
- Vertigo
- Disequilibrium
- Pre-syncope
- Light-headedness
Vertigo
- Benign paroxysmal positional vertigo (BPPV)
- Occurs due to problems in the heavy calcium particles (otoliths) present in the vestibular labyrinth
- Transient, episodic vertigo is induced by head position changes.
- most commonly post semicircular canal
- usually self-limiting, lasting up to 6/52
- vertigo lasts seconds - associated with movement

- Meniere's disease
- idiopathic by definition. Syndrome may develop secondary to trauma, infection, autoimmune disorders, endocrine disease, medications etc
- criteria:
- vertigo ≥2 episodes lasting 20mins up to 12/12
- documented low to mid frequency sensorineural hearing loss
- fluctuating hearing loss, tinnitus or pressure in affected ear
- other causes excluded
- vertigo lasts hours
- Migrainous vertigo (vestibular migraine)
- one of most common causes of vertigo
- vestibular syndrome alongside other migraine symptoms such as headache, nausea, sensitivity to light and sound and aura
- headache not always present
- Criteria:
- ≥5 episodes
- present or PHx migraine
- vestibular symptoms (vertigo or dizziness) lasting five minutes - 72 hours
- the concurrence of migraine headache or other migraine associated symptoms in at least half of the episodes.
- vestibular neuronitis
- most likely viral with some caused by latent HSV1 reactivation in vestibular ganglia
- vertigo, nausea, vomiting, nystagmus (Vestibular syndrome)
- vertigo may last days, weeks
- labyrinthitis
- usually viral cause
- Vestibular syndrome plus sensory deafness and tinnitus
- vertigo may last days, weeks
Central vs Peripheral
| Peripheral | Vertigo | • Intermittent and positional • Vertigo stops with visual fixation |
|---|---|---|
| Nystagmus | • delayed in onset rotatory or horizontal prominent if vertigo is present adaptive | |
| Other | • more likely to be associated with hearing loss, tinnitus | |
| Central | Vertigo | • Non-positional • does not stop with visual fixation |
| Nystagmus | • immediate or delayed in onset rotatory, horizontal, or vertical, not adaptive | |
| Other | • more likely to have other Brainstem signs and symptoms |
Self limiting acute vestibular syndrome vs stroke
HINTS tests
- Head Impulse tests Vestibulo-ocular reflex (VOR) - disturbed in vestibular disease but not stroke
- abnormal response is indicated by an inability to maintain fixation during head rotation with a corrective gaze shift after the head stops moving.
- the Head Impulse involves high acceleration by low amplitude rotation of the head
- Nystagmus
- multi directional nystagmus has central cause
- ie. gaze to Left causing L nystagmus and gaze to R causing nystagmus to R = central origin
- Skew - when vertical alignment of the eyes is different. Can be made to more obvious by covering then uncovering one eye to reveal realignment
Hallpike-Dix Manoeuvre
- sitting midway on flat exam table, instructed to look ahead at all times, examiner turns pt's 45o head to side and rapidly moving pt back to supine position with head over the edge of the table. Observe of 30sec.
- Rotatory nystagmus is seen if the superior semicircular canal is involved (most common)
- Horizontal nystagmus is seen if the lateral semicircular canal is involved
- upbeating with rotatory nystagmus(top pole rotates toward under-most affected ear) is seen if post semicircular canal involved
Epley Manoeuvre
- generally used to treat vertigo caused by BPPV involving the posterior semicircular canal, the most common type of BPPV
(View Manoeuvre)close

Management
- Benign Paroxysmal Positional Vertigo:
- Epley manoeuvre particlulary for post semicircular canal. Brandt-Daroff exercises
- medication generally not helpful
- Meniere's disease:
- symptomatic - prochlorperazine,
- Histamine agonits eg betahistine can be helpful (?increases circulatory flow to cochlear or my inhibit vestibular nuclei activity)
- steroids can be helpful
- Migrainous vertigo:
- treatment as with other migraine types
- difficult to differentiate from Meniere's disease as episodic dizziness with auditory auras make the two similar
- important to have preventative med's eg amitriptyline, propranolol, candesartan, flunarizine
- Vestibular neuronitis:
- prochlorperazine or antihistamine
- Cochrane review - steroids not thought to be useful immediately or long term
- Labyrinthitis:
- usually viral, so supportive med's only
Presyncope
- Cardiovascular causes of dizziness include arrhythmias, myocardial infarction, carotid artery stenosis, and orthostatic hypotension
- medications - especially but not only cardiovascular med's
Disequilibrium
- stroke, TIA, VBI (Quick View)close
VBI
Vertebro-basilar Insufficiency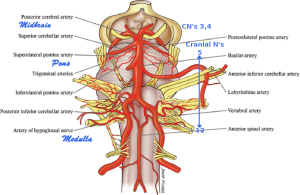
 Brainstem circulation with Cranial Nerve approximation
Brainstem circulation with Cranial Nerve approximation
1 a clinical syndrome caused by transient ischaemia of the vertebrobasilar circulation, formed by the vertebral and basilar arteries, which forms the posterior circulation of the brain.
 vertebrobasilar arteries supply the cerebellum, medulla, midbrain, and occipital cortex
vertebrobasilar arteries supply the cerebellum, medulla, midbrain, and occipital cortex
most commonly caused by atherosclerosis and/or embolism. Embolism is uncommon in vertebral arteries
Presentationvertigo, dizziness,syncope, drop attacks
diplopia, visual field deficits, blindness
ataxia, imbalance, dysmetria are common
dysphagia, dysarthria are common
contralateral weakness
ipsilateral cranial N involvement when present
Vertebral artery STROKE is associated with a variety of syndromesLocked in syndrome
Lateral medullary syndrome
Internuclear ophthalmoplegia
Cerebellar infarction
Medial medullary syndrome
Posterior cerebral artery occlusion
Management
as for TIA in general although vertebral artery TIA/stroke less commonly atherosclerotic in nature and endarterectomy/stent therefore less likely. The more distal from the brain the more likely.
angioplasty for basilar artery disease is not uncommon
as for TIA, prevention is key and risk stratification is central
control of hypertension, diabetes
management of arrhythmias
lipid lowering
blood thinners
References include:
https://radiopaedia.org/articles/vertebrobasilar-insufficiency?lang=gb
https://www.ncbi.nlm.nih.gov/books/NBK482259/
http://www.dizziness-and-balance.com/disorders/central/strokes/tia.html
and acoustic neuroma need excluding - Poor vision commonly accompanies a feeling of imbalance
- Parkinson disease, peripheral neuropathy, and any musculoskeletal disorders that may affect gait
- benzodiazepines and tricyclic antidepressants
- age

Light-headedness
- anxiety is common
- depression and alcohol intoxication
- hyperventilation
References include:
https://www.aafp.org/afp/2010/0815/p361.html
https://www.enteducationswansea.org/acute-vestibular-syndrome
https://emedicine.medscape.com/article/884261-clinical#b4
https://entokey.com/3-6-vertigo/
https://cks.nice.org.uk/vestibular-neuronitis#!scenario
https://www.emra.org/emresident/article/hints-exam/
https://www.migrainetrust.org/about-migraine/types-of-migraine/migraine-and-vertigo/
https://www.dizziness-and-balance.com/disorders/unilat/vneurit.html
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096243/
Approach to acute vertigo - practical neurology